|
"What are the chances
of survival on the operating table?" the lady owner
wiped her reddened eyes. Her Maltese had swallowed a
chicken wing and had emergency night consultation at Vet
1. Surgery was quoted at $1,000. I estimated that Vet
1's fees would go up to $2,000 - $3,000, inclusive of the
emergency night consultation and medication.
3 X-rays of the
lateral view of the stomach by Vet 1 showed a chicken
humurus (forearm) bone mostly in the oesophagus (gullet)
and partly in the stomach.
"Why did vet 1 take 3 X-rays of the same view?" I asked
her as I was puzzled.
To see whether the
bone had moved into the stomach". Would the bone
move, given time? I doubt it as the end inside the
gullet was much larger in diameter. In any case, the dog
vomited around 40 ml of white frothy saliva onto my
consultation table twice and wanted to vomit more. This
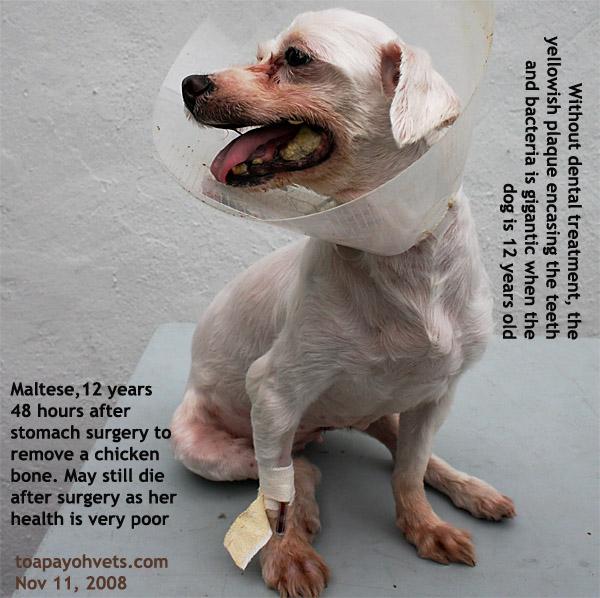
12-year-old was in poor health. Heart disease was bad
enough. She had gum disease (large plaques encasing
teeth) and infection of the womb (pyometra).
There was no time to wait for the bone to move into the
stomach. But what are her chances of survival on the
operating table? I said, "Due to her old age, her heart
disease, infection of the womb, fever and general poor
ill, I would give her a 5%".
I prefer not to operate on high risk anaesthetic cases
as no good will ever comes out of it if the dog dies on
the operating table.
But her friend had referred her to me as I was once a
horse veterinarian. "If you can operate on a horse which
is such a large animal, you can operate on a dog," the
lady said.
It was difficult situation for the owner too. If the dog
was not operated, the dog would die a painful death from
continuous vomiting, fever and starvation as food could
no longer pass into the stomach. If her dog was operated
a 5% chance of survival was not good enough. She took
some pictures of her dog with her camera phone.
VETERINARY ANAESTHESIA AND SURGERY
1. No injectable sedatives or anaesthetics were used
so as not to depress the cardio-respiratory system.
There are good injectable anaesthetics but they require
topping up to achieve surgical anaesthesia.
2. Was it possible to scope and take out the chicken
bone from the mouth and gullet? A flexible scope with a
forceps to grip the bone? If there was such a
scope, it would cost a lot of money. Here, the owner
wanted the least cost surgery.
3. How to get the bone out then? The bone was trapped by
the gastro-esophageal sphincter muscle. Would it be
possible to pull it out of the gullet via the sphincter?
Would there be traumatic injury and bleeding to the
sphincter?
4. What surgical approach would be used? There was only
one simple approach - via the stomach. I could not feel
the bone on palpation of the stomach. Therefore, it must
be sticking into the stomach by a short length only.
X-rays showed it was around 1/4 inside the stomach.
VETERINARY ANAESTHESIA
PROBLEM 1. Difficult Airway/Aspiration Risk
Isoflurane gas by mask was given. When the dog was
sleepy, I opened her mouth to intubate. Her epiglottis
was covered by white foamy saliva. It was like a smoke
screen. No opening of the epiglottis could be seen and
therefore I could not put in the endotracheal tube and
therefore could not maintain the surgical anaesthesia
with gas.
"Too much saliva make intubation impossible," I said to
my assistant Aung. "What is the solution?"
Revert to the use of injectable anaesthetic? This seemed
to be the only choice. Injectable anaesthetic would be
very risky as there was no rapid means of reversal
should the dog's heart fail.
Aung was ready to get the injectable anaesthetic.
"Wait," I said. "I will hang the dog upside down, slap
her chest to get the chicken bone to drop out." I
held the Maltese by her hind legs and slap her thorax 4
times.
Aung looked at me in surprise and probably wondering
whether I had gone nutty. No chicken bone would ever
drop out just like that. It was just physiologically
impossible. Aung was a serious man. He seldom talked
more than necessary to me but he said, "It is not
possible to get the bone out this way."
Hanging the Maltese upside down was to get the frothy
saliva out of the epiglottis and out of the mouth. But I
did not tell Aung and so he really thought that I had
intended to get the chicken humurus bone out by simply
hanging the dog upside down.
The difficult airway/aspiration risk problem was
resolved. The saliva was gone and I was able to intubate
the dog.
VETERINARY SURGERY
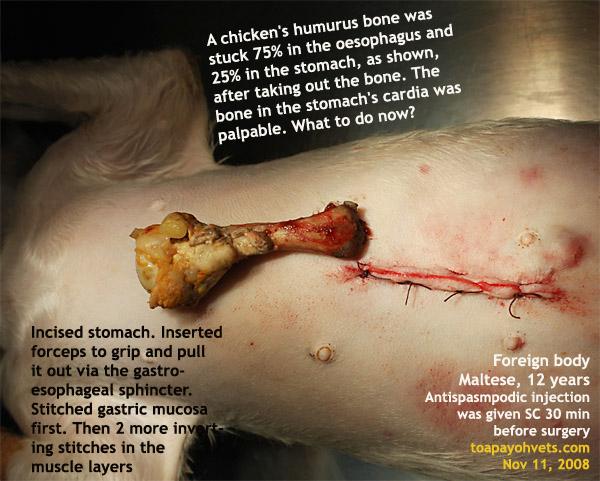
PROBLEM 2. Chicken bone's end was larger inside the
oesophagus than inside the stomach (see X-ray).
Would pulling the chicken bone out traumatise the
gastro-esophageal sphincter?
"Can the chicken bone be split into 2 long halves?"
I tested Aung who had a big passion for veterinary
medicine and surgery. Aung must have thought I was nutty
again and shook his head. The bone end inside the
stomach was felt. The problem was that it was a smaller
diameter than the end inside the gullet. Would pulling
it out via the stomach damage the sphincter and cause
bleeding?
The dog must be trying to vomit out the bone end inside
the stomach but the sphincter would not permit it as it
tightened round the bone.
From my horse medicine, I used anti-spasmodic drugs for
impaction colic. 30 minutes before surgery, I had given
this dog an anti-spasmodic injection so as to
relax the sphincter muscle. Antibiotic was given
too.
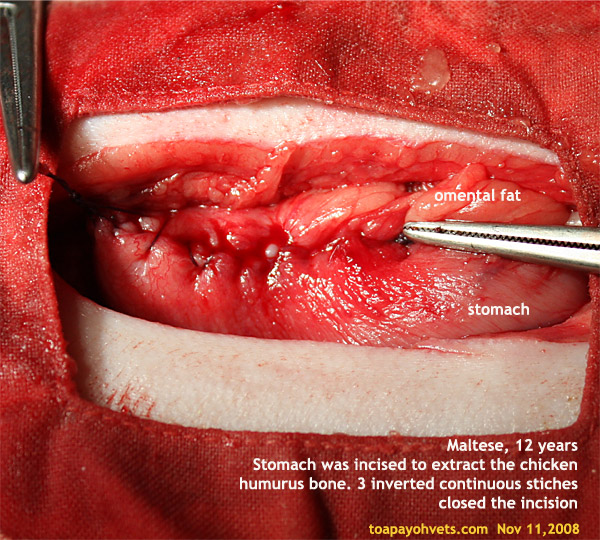
I put the artery forceps into the stomach incision, felt
and gripped the end of the bone and pulled it out at one
go. The bone came out easily. 2 pieces of meat came out
too and I was careful not to let them contaminate the
peritonium by removing them fast.
The gastric mucosa was purplish as I sutured it with an
inverted continuous suture. Some blood flow to it must
have been cut off, otherwise it should be pinkish.
Fortunately, there was no delay in the surgery. Two
inverted continuous suture closed the stomach wall. The
dog woke up in a daze but was all right.
The dog had no
problem during anaesthesia. Her tongue was a healthy
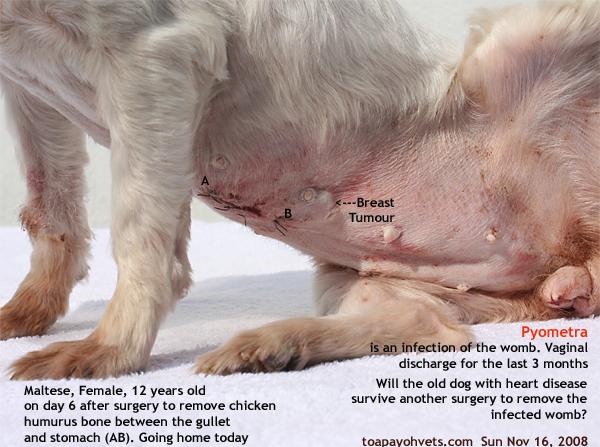
pink colour. She went home at day 6 after surgery. Once
home, she was active and ran to greet her owners when
they come home from work. So she started to pant.
She was warded on
day 8 for observation and treatment of her heart
disease.
She was still bleeding from the pyometra infection and
had this bleeding for at least 3 months. The
only cure was surgery to spay her.
I feel that another
veterinarian should do the spay as it is not good as this dog
may die on the operating table. And chances are very high
that she would die. Why should I tempt fate a second
time? |